

Sponsored Content
“No matter how many do it wrong, doesn’t make it right.”
For Edwin Zinman, DDS, JD, the presence of a crowd doesn’t add a sense of comfort – and certainly not a legal defense.
As a former periodontist and now practicing lawyer, Dr. Zinman has been involved in hundreds of cases of breaches in infection control, and perhaps most notably, those involving dental unit waterline contamination.
While at times, this has put Dr. Zinman in opposition to dental practices in litigation, it has always been with the hope of ensuring the best dental practices rise to the top.
His unique perspective both as a lawyer and a dentist provides invaluable insight to the rest of the profession. But as with many industry educators, it often starts with the basics – the standard of care.
“All reasonable and careful dentists should be following the 2003 CDC (Centers for Disease Control) guidelines for infection control as these recommendations have remained unchanged for 16 years.”
The standard of care, what a reasonable and prudent dentist would do in the same or similar circumstances, according to Dr. Zinman, does not mean what a few good buddies from dental school do or even what the majority of dentists do. As he says often, “No matter how many do it wrong, does not make it right.” The standard of care is what a reasonable and prudent dentist would do, and after almost two decades of well-established scientific basis, following the CDC guidelines on infection control, is what reasonable and prudent dentists would do.
Failing to measure up to that standard opens up a world of liability.
A SECOND LOOK AT THE CDC’S DENTAL WATER QUALITY GUIDELINES
The CDC’s Guidelines For Infection Control in Dental Health-Care Settings – 2003 outline the historical and clinical implications involved with dental unit waterline contamination as well as provides practical recommendations to prevent infection (see figure 1).
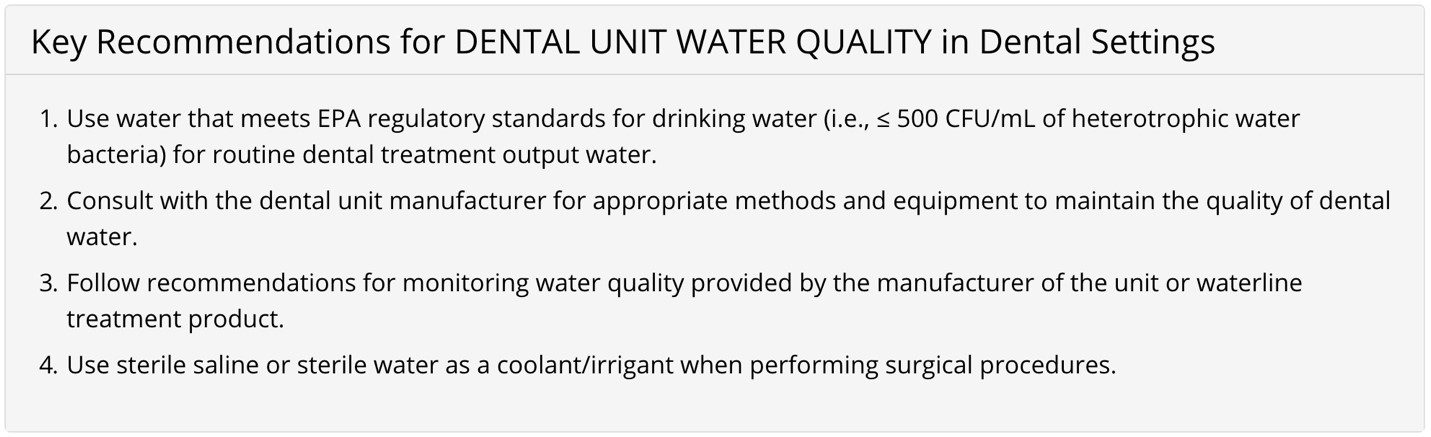
Figure 1: United States Centers for Disease Control; Infection Prevention and Control in Dental Settings; Summary of Infection Prevention Practices in Dental Settings; “Dental Unit Water Quality”; June 18, 2018; https://www.cdc.gov/oralhealth/infectioncontrol/summary-infection-prevention-practices/dental-unit-water-quality.html.
These recommendations direct each practice to use sterile water and sterile delivery systems for surgery as well as treat dental unit water to ensure it is less than the EPA standard for drinkable water (≤ 500CFU/mL), and verify the effectiveness of the treatment protocols through periodic waterline testing.
THE RISKS OF NON-COMPLIANCE
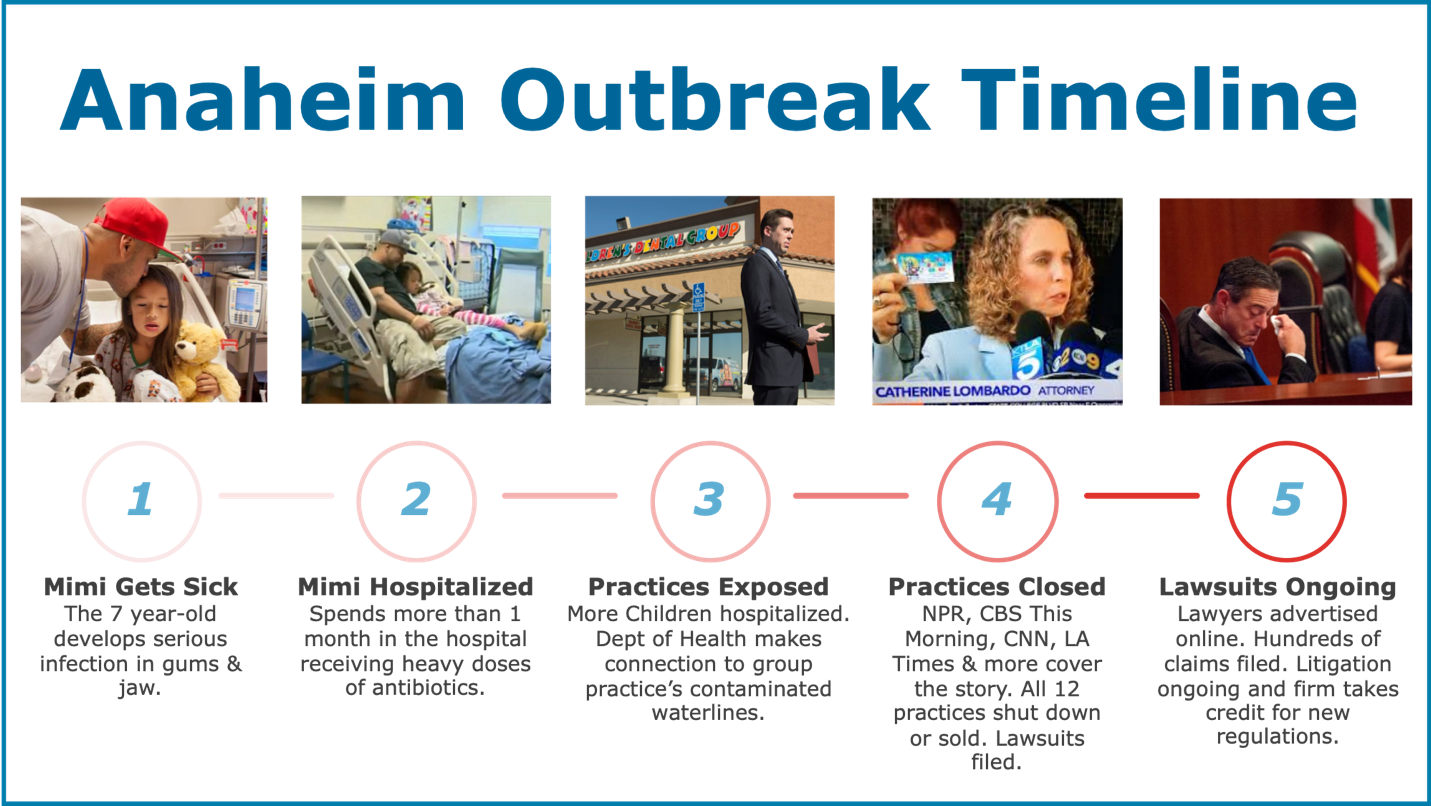
Since these guidelines were published, dental water has come under much greater scrutiny, particularly due to two outbreaks of mycobacterium abscessus in Atlanta, Georgia and Anaheim, California that resulted in well over 100 healthy pediatric patient infections in 2015 and 2016. Currently, at least 150 lawsuits were filed against the ownership group involved in Anaheim.
©ProEdge Dental Water Labs
But while these two cases grabbed the headlines, lesser known infections linked to dental unit waterline contamination still do their damage.
“I’ve been litigating these cases for a couple decades,” says Dr. Zinman. “Many of these legal cases are settled with confidentiality agreements so they are not published in literature purposely so there is no public knowledge.”
The first trial in the Anaheim case is scheduled for January, 2020. Should the ruling be in favor of the plaintiffs, this case will again get widespread attention.
“The public will ask their dental office if they are complying with the infection control guidelines.” says Dr. Zinman.
3 WAYS TO PROTECT YOUR DENTAL SERVICE ORGANIZATION
Each dentist will be held to the standard of care, which means complying with the CDC guidelines as noted above. To protect both your patients and your practices, take these three steps:
1. Get Educated
For developing a comprehensive and protective waterline protocol capable of protecting your organization, Dr. Zinman suggests starting with three important documents.
First, thoroughly review and understand the CDC Guidelines For Infection Control in Dental Health-Care Settings – 2003. Establish protocols for each of the key recommendations surrounding dental water quality.
Second, read Dental Unit Water Quality: Organization for Safety, Asepsis and Prevention White Paper and Recommendations– 2018 by Shannon Mills, DDS, Nuala Porteous, BDS, MPH, and Jeff Zawada, PhD. This more recent work reinforces the CDC’s position while also providing additional insights based on the latest in dental water research and technology.
And lastly, download the CDC’s Infection Prevention Checklist for Dental Settings: Basic Expectations for Safe Care. This checklist can help systematically assess compliance within each office and help direct your organization in developing standard operating procedures for each aspect of infection control.
©ProEdge Dental Water Labs
2. Get Documented Records
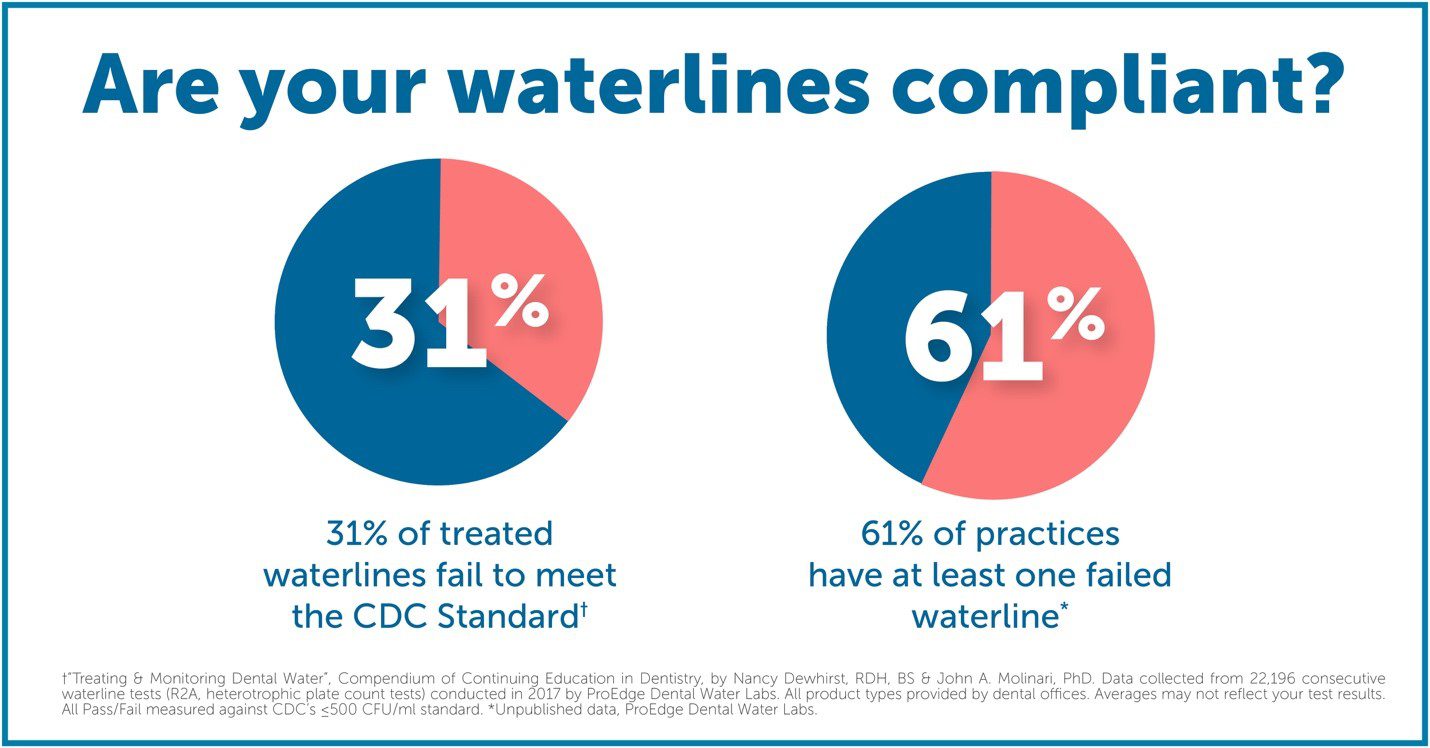
When it comes to dental waterlines contamination, having a treatment in the water does not equate compliance. Each office needs objective proof their protocol meets or exceeds the EPA standard for potable water (≤500 CFU/mL).
“The three R’s of malpractice prevention are records, records, and records,” says Dr. Zinman.
“Testing is necessary to demonstrate compliance. There can be failures – particularly created by staff – so if a dentist does not know if they have adequately followed the protocol, there is no objective proof that particular dental office is complying with the guidelines.”
The CDC, ADA, FDA, and OSAP suggest DSOs consult with their dental unit and treatment product manufacturer to determine recommended testing frequency. If no specific frequency is available, OSAP recommends testing monthly until two consecutive passing cycles, and then quarterly.
Keep records of waterline test results for at least 5 years.
3. Get a Partner
What protocol is going to scale as we grow? What products are most effective? How are we going to make sure staff comprehend the importance of waterline maintenance? Who’s going to track test compliance and results?
Great questions without easy answers. If resolving waterline contamination was easy, it would have been solved back in 2003. But biofilm is complex, dental waterline technology is ever-changing, and large treatment investments need to yield passing test results.
But easy isn’t the point anyway.
As Dr. Zinman says, “One should not be risking patient health for expediency. We do many things in dentistry just for protections because we are to act in the best interest of the patient. That’s our legal and ethical obligation and that’s what patients expect and that’s what patients deserve.”
And that perspective is what we’re all about.
ProEdge Dental Water Labs is the most experienced dental water testing laboratory in the world. Every year, we test more water, collect more real-world efficacy data, and consult with more practices to get them to CDC-compliant water than anyone in the industry.
Our team has helped some of the largest DSOs in the world develop cost-effective protocols, train staff, track progress, and ensure compliance. ProEdge doesn’t just tell you what you want to hear; we provide the scientific and research supported answers you need to protect your patients and your practices for the long-term.
To take a free test drive of ProEdge services or for a protocol consultation, contact Kelley Birschbach, VP of Marketing & Sales, at KelleyB@ProEdgeDental.com.

Dr. Edwin Zinman received his DDS from the University of Pittsburgh School of Dentistry and his  certificate in periodontics and oral medicine from NYU. After practicing periodontics in New York and San Francisco and continuing his teaching at UCSF Department of Periodontics, Dr. Zinman graduated UCSF Hastings College of Law. Dr. Zinman has lectured several hundred times to local, state and national dental societies, and legal associations. His authorship includes chapters in 12 different dental textbooks, articles in the Journal of American Dental Association, California Dental Association and columnist in Dental Management, in addition to legal journals.
certificate in periodontics and oral medicine from NYU. After practicing periodontics in New York and San Francisco and continuing his teaching at UCSF Department of Periodontics, Dr. Zinman graduated UCSF Hastings College of Law. Dr. Zinman has lectured several hundred times to local, state and national dental societies, and legal associations. His authorship includes chapters in 12 different dental textbooks, articles in the Journal of American Dental Association, California Dental Association and columnist in Dental Management, in addition to legal journals.


